SBM-R approach was implemented in the context of major structural challenges facing the health system, including chronic staff shortages and turnover, insufficient infrastructure, and community mistrust owing to the 2014-16 Ebola epidemic. The findings are categorized into – process and engagement, performance drivers including clinical performance, managerial performance, and equipment, supplies, and infrastructure.
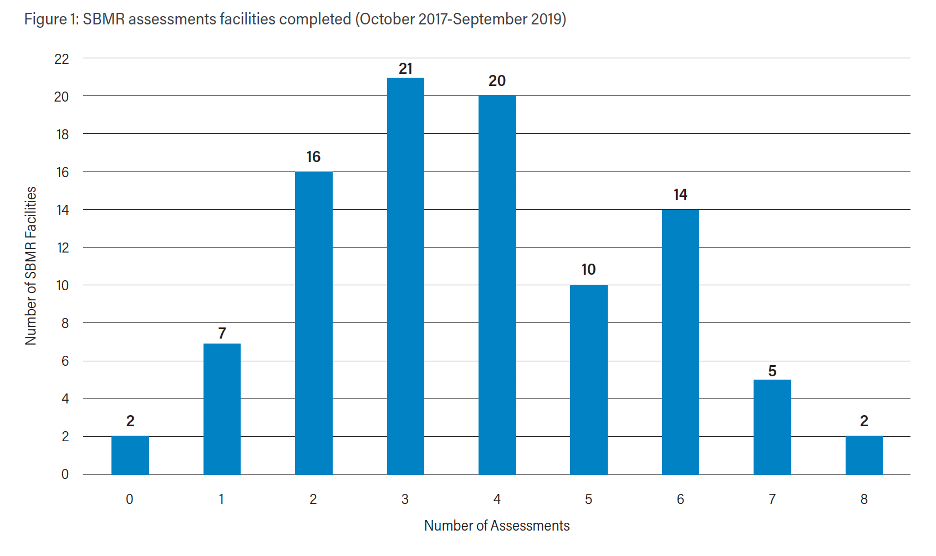
Process and Engagement: The SBM-R process occurred in two steps – (1) a regular self-assessment carried out at the facility-level by a team of providers, senior managers, COSAH representatives, and community members. The second step involves the requests made by the facility to be externally evaluated by the national committee. The facility’s performance is based on the external review on a performance threshold and provided ‘star’ ratings. For instance, if the facility receives 80% or greater, it receives one star; a second star when the facility demonstrates performance for at least 86% of the standards. Of the 272 HSD-supported facilities, 97 implemented the SBM-R program, and about half of these facilities earned one or more stars. The 97 SBM-R facilities implemented the approach, on average, for four years. A wide variation was noted in the frequency of facilities’ level of engagement – 47% of all SMB-R facilities were considered to have low engagement with three or fewer assessments from 2017-2019.
Performance drivers: There were 3 performance drivers noted including clinical performance, managerial performance, and equipment and supplies.
Clinical Performance: The case study demonstrated marked improvements in scores for infection prevention and control practices with a wide range from a 25 to 70 percentage point increase. Other large improvements in clinical practice were attributed to obstetric interventions, though more improvements were needed for respectful care and complex health interventions. While family planning performance standards generally improved across the case study facilities, challenges in providing evidence-based information on specific family planning methods continued to be noted.
Managerial Performance: Several managerial issues were noted including poor client-provider communication; low availability of information, education, communication materials; lack of job descriptions for staff; and long wait times for clients.
Equipment, Supplies, and Infrastructure: Many of the facilities in the case study also faced challenges related to receiving supplies such as scales, blood pressure gauges, and examination tables. The facilities’ capacities to conduct sterilization and waste management were an issue due to a lack of disinfectants, antiseptics, and personal protective equipment. Overall, management was a critical player in alleviating these issues.

